
Tirzepatide
Also known as: Zepbound, Mounjaro, LY3298176
Overview
Tirzepatide is an FDA-approved first-in-class dual GIP/GLP-1 receptor agonist peptide that simultaneously activates both glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors. The addition of GIP receptor agonism to GLP-1R activation produces superior weight loss outcomes compared to GLP-1 monotherapy alone. The SURMOUNT-1 trial demonstrated 20.9% average body weight reduction with tirzepatide 15 mg, surpassing semaglutide results in head-to-head SURMOUNT-5 trial. Approved for T2D (Mounjaro, 2022) and obesity (Zepbound, 2023).
Mechanism of Action
Tirzepatide activates both GIP-R and GLP-1R through complementary pathways. GLP-1R activation in the hypothalamus, pancreas, and periphery drives appetite suppression, incretin insulin secretion, and slowed gastric emptying. GIP-R activation enhances insulin response and appears to reduce some GLP-1 nausea side effects by paradoxical peripheral mechanisms. Together these produce superior reductions in respiratory quotient (RQ), indicating greater fat oxidation versus GLP-1 alone. Tirzepatide shows stronger suppression of lipid synthesis genes (Scd1, Fasn) in liver than semaglutide.
Potential Benefits
- FDA-approved for T2D (Mounjaro) and obesity (Zepbound)
- ~20.9% average body weight reduction in SURMOUNT-1 at 15 mg
- Superior to semaglutide in SURMOUNT-5 head-to-head trial
- Significant HbA1c reduction (2.24% vs semaglutide in SURPASS-2)
- Improved cardiovascular risk factors including blood pressure
- Reduced fatty liver disease markers
- Potential heart failure benefits (SUMMIT trial)
Dosage Protocols
The following reflects doses used in published research studies. This is not medical advice. Consult a qualified healthcare professional.
| Typical Range | 2.5-15 mg/week |
| Beginner | 2.5 mg/week for 4 weeks |
| Intermediate | 5-10 mg/week |
| Advanced | 12.5-15 mg/week (FDA-approved max for obesity) |
| Cycle Duration | Ongoing therapeutic; titrate up every 4 weeks as tolerated |
| Cycle Off | Not designed for cycling; weight regain occurs after discontinuation |
FDA titration for Zepbound: 2.5 mg/week → 5 mg (wk 5) → 7.5 mg (wk 9) → 10 mg (wk 13) → 12.5 mg (wk 17) → 15 mg (wk 21). GI side effects typically diminish after titration period.
Use our Reconstitution Calculator to determine exact syringe units for your protocol.
Routes of Administration
Subcutaneous Injection High — systemic distribution
Most common administration route for research peptides. Inject into abdominal fat, thigh, or upper arm. Rotate sites. standard research dose.
Intramuscular Injection High — with slightly faster onset than SC
Alternative route when deeper delivery or faster absorption is desired. Less commonly used than SC for most research peptides.
Read our full Routes of Administration Guide for detailed comparison of all delivery methods.
Stacking Protocols
Popular research stacks involving Tirzepatide:
Metabolic Health Stack
Combines Tirzepatide with MOTS-c (mitochondrial metabolism) and AOD-9604 (lipolysis) for metabolic optimization.
Explore our complete Peptide Stacking Guide for more combinations and safety considerations.
Reconstitution
| Typical Vial Size | 2.5mg, 5mg, 7.5mg, 10mg, 12.5mg, 15mg auto-injector pens |
|---|---|
| BAC Water | N/A — supplied as pre-mixed solution |
| Storage | Refrigerate at 2-8°C; may store at room temperature (≤30°C) up to 21 days |
| Shelf Life | 24 months unopened; 21 days after removal from refrigeration |
Need exact syringe measurements?
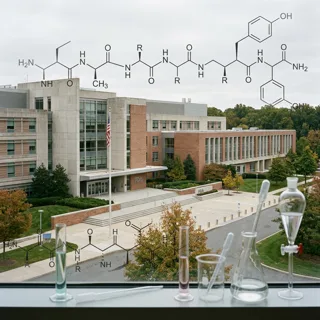
Amino Acid Sequence
Modified GIP/GLP-1 dual agonist with C20 fatty diacid moiety for albumin binding (39 amino acids)
Side Effects & Safety
- Nausea, diarrhea, constipation (most common, dose-dependent)
- Decreased appetite
- Vomiting
- Higher discontinuation rate than semaglutide at high doses
- Lean mass reduction alongside fat loss
- Gallbladder disease risk
Safety & Contraindications
This information is for educational purposes only. Consult a qualified healthcare provider before using any peptide.
Personal or Family History of Medullary Thyroid Carcinoma or MEN 2
Pregnancy / Lactation
Bleeding Disorders
Active Skin Infection at Injection Site
Drug Interactions
- Oral Medications (general):
FDA Safety Information
FDA Boxed Warning: Risk of thyroid C-cell tumors. Contraindicated in patients with personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
Pharmacokinetics
| Half-Life | ~5 days |
|---|---|
| Storage | Pens/vials: refrigerate at 2-8°C. Once in use, can be stored at room temperature (up to 30°C) for up to 21 days. Do not freeze. |
Synergistic Compounds
The following compounds have been studied alongside Tirzepatide for potential complementary or synergistic effects:
Learn More
References & Further Reading
Latest News & Research
View all articles →
FDA Staff Reviewers Say ‘No’ to 7 Compounded Peptides Ahead of July PCAC Vote
FDA staff reviewers urged against adding seven popular peptides to the 503A bulks list ahead of the July PCAC meeting, citing weak human data and safety uncertainty.

FDA reviewers urge ‘no’ on BPC-157, TB-500, MOTS-c ahead of July 2026 compounding vote
FDA reviewers’ June 29 briefings recommend against listing seven popular peptides for 503A compounding, citing limited human data and immunogenicity risk.

Medicare Starts Paying for Obesity Drugs Today — Bridge Program Opens $50 Access for Millions
Medicare's new $50 Bridge program covering Wegovy, Zepbound, Foundayo, and oral Wegovy for obesity launched July 1 — the first Medicare weight-loss benefit.
FDA staff urges caution on compounded peptides ahead of July advisory meeting
Ahead of the July 23–24 Pharmacy Compounding Advisory Committee meeting, FDA staff briefings recommend against listing seven popular peptides for compounding.