
What Was Published
A team led by Ali Güler at the University of Virginia has identified the specific brain circuit through which the new oral GLP-1 weight-loss drugs turn down cravings for high-calorie food. The paper appeared in Nature on May 6, 2026. Its formal title is "A brain reward circuit inhibited by next-generation weight-loss drugs in mice." First author is Elizabeth N. Godschall; the DOI is 10.1038/s41586-026-10444-4. The work was funded by the National Institutes of Health, which published a release the same day; the University of Virginia put out its own summary.
The headline finding is anatomical. Oral small-molecule GLP-1 receptor agonists — orforglipron (Eli Lilly's recently approved tablet, brand name Foundayo) and danuglipron (Pfizer's discontinued oral candidate) — reach a population of GLP-1-receptor-expressing neurons in the central amygdala. Activating those neurons suppresses dopamine release into the nucleus accumbens and reduces eating for pleasure. Deleting the receptor from that one population, while leaving the rest of the brain's GLP-1 receptors intact, blunts the drugs' effect on palatable food specifically and leaves the effect on standard chow largely alone.
That clean dissociation between homeostatic and hedonic feeding, in a single anatomical site, is what makes this a paper rather than a press release.
Key Facts
- Paper: Godschall EN, Gungul TB, Sajonia IR, et al. Nature, May 6, 2026. DOI 10.1038/s41586-026-10444-4.
- Senior author: Ali D. Güler, University of Virginia.
- Drugs studied: Liraglutide (peptide, injectable), danuglipron (small molecule, oral, Pfizer-discontinued), orforglipron (small molecule, oral, Eli Lilly, FDA-approved April 1, 2026 as Foundayo).
- Why a humanized mouse: Orforglipron and danuglipron bind human GLP-1 receptor but not the mouse version. The difference is a single amino acid — tryptophan at position 33 in humans, serine in mice. The team engineered mice with humanized GLP-1 receptors before any of the experiments could work.
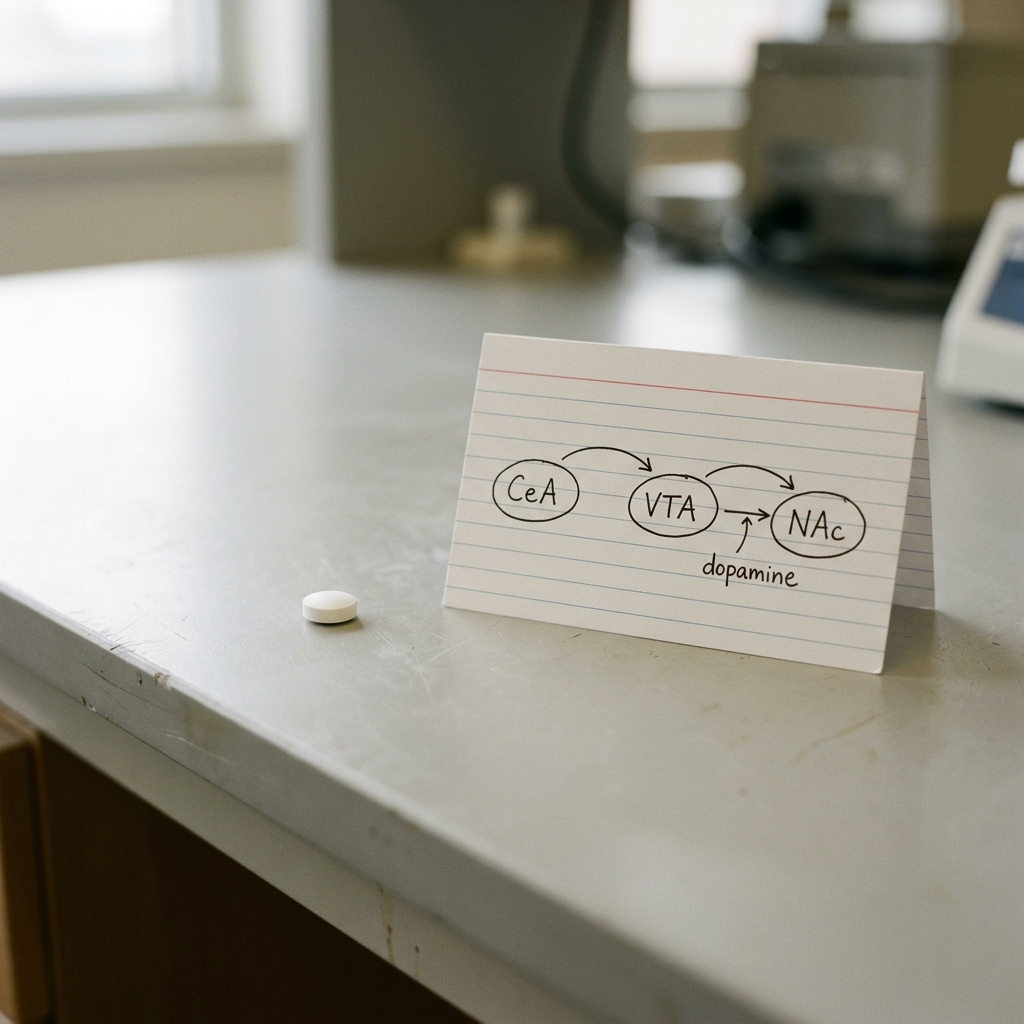
- The circuit: Central amygdala (CeA) GLP-1-receptor neurons → ventral tegmental area (VTA) → nucleus accumbens (NAc) dopamine.
- Behavioral dissociation: Re-expressing the human receptor only in the CeA reduces high-fat diet intake without affecting standard chow intake. Re-expressing it only in the hypothalamus (DMH) does the opposite. Re-expressing it only in the hindbrain (NTS-AP) reduces both.
- Conditional knockout: Deleting GLP-1 receptor in the CeA blunts liraglutide's anorectic effect on palatable food, without affecting its effect on standard chow.
- Dopamine measurement: All three drugs (liraglutide, danuglipron, orforglipron) attenuated nucleus accumbens dopamine transients during high-fat-diet consumption.
- Therapeutic implications: A defined circuit for reward suppression, which the authors suggest could be relevant to clinical observations of reduced alcohol and cannabis use among GLP-1 users.
- Caveat: Findings are in mice. Human data on these specific mechanisms remain inferential.
Why This Paper Matters
The clinical observation came first. People taking GLP-1 receptor agonists for diabetes or weight loss reported losing interest in food in a way that did not fit the usual story of "feels full sooner." Many also reported drinking less alcohol. Some quit smoking. A subset described a flatter overall mood — less excitement about things they used to enjoy. None of this was what GLP-1 drugs were originally supposed to do.
For a decade, the mechanistic story for these drugs has been built around the hindbrain. Receptors in the nucleus tractus solitarius and area postrema in the brainstem detect GLP-1, signal fullness, and produce the nausea that is the class's most common side effect. Receptors in the hypothalamus participate in longer-term regulation of food intake. That story explains a lot. It does not explain why someone taking semaglutide loses interest in their second glass of wine, or why a long-term user reports finding food less rewarding in a way that has nothing to do with feeling full.
The Güler paper provides a mechanistic substrate for those observations. There is a specific population of neurons in the central amygdala that expresses the GLP-1 receptor. Those neurons project, directly or indirectly, to the dopamine system. The drugs reach them. The drugs activate them. The activation reduces dopamine release in the reward circuit. That changes how rewarding food, and possibly other rewards, feel.
The work is rigorous in a way that small-molecule GLP-1 pharmacology has not previously been able to be. Most prior studies used liraglutide and semaglutide, which bind the mouse GLP-1 receptor reasonably well. The new oral small molecules do not. Without the humanized mouse model, you cannot study orforglipron or danuglipron pharmacology in a mouse at all — the receptor does not bind the drug. The Güler team built that model. Then they built three more conditional re-expression models to localize the receptor to specific brain regions. The result is the cleanest dissection of GLP-1 reward effects in any species to date.
The Tryptophan Problem and Why It Held the Field Back
Drug discovery for non-peptide GLP-1 receptor agonists ran into the same wall every program hit. The molecules bind human GLP-1 receptor with low-nanomolar potency. They do nothing in mice. The reason, worked out in detail by Pfizer and Lilly chemists in 2020, is structural. The small-molecule agonists dock into a pocket near the receptor's extracellular surface, and one of the contacts they need is the indole side chain of tryptophan at position 33. Human GLP-1 receptor has tryptophan there. Mouse GLP-1 receptor has serine. Serine's small hydroxyl side chain cannot make the same contact. The receptor still works for endogenous GLP-1, which binds elsewhere on the protein; it does not work for the small molecules.
This is a recurring problem in pharmacology. Receptor sequences diverge enough between mouse and human that drug screens against the human target can land on molecules that hit a feature mice do not have. The standard workarounds — non-human primate models, in vitro pharmacology only, or knock-in of the human receptor — each have costs. The Güler team chose the knock-in route and went further. They built not just a humanized GLP-1 receptor mouse, but conditional versions in which the human receptor is expressed only in specific cell populations defined by Cre recombinase drivers.
Once you have those tools, you can do experiments that are otherwise impossible. Inject orforglipron into a mouse whose only humanized GLP-1 receptors are in the central amygdala. If the drug suppresses palatable food intake, the central amygdala is sufficient. If you knock out the same receptor specifically in that region in an otherwise-humanized mouse, and the drug stops working on palatable food, the central amygdala is necessary. The paper does both. That is what gives the central-amygdala story its weight.
The Circuit, Concretely
The relevant GLP-1-receptor neurons live in the lateral subdivision of the central amygdala. They project through several intermediate steps to the ventral tegmental area, the dopamine source for most of the reward circuit. The Güler team used a combination of anterograde tracing, monosynaptic rabies tracing, fiber photometry, and optogenetics to put the wiring diagram together.
The functional sequence is short. Orforglipron or danuglipron enters the brain and activates GLP-1 receptors on the relevant central amygdala neurons. Those neurons increase their firing. Their downstream effect on the VTA reduces the firing of midbrain dopamine neurons during a palatable meal. Less dopamine reaches the nucleus accumbens. The nucleus accumbens is where the brain's reward signal is most directly read out. With less dopamine arriving there, the high-calorie food does not register as strongly rewarding, and intake drops. The team measured the dopamine transient directly using genetically encoded dopamine sensors in the nucleus accumbens. The signal was reduced under all three drugs — including injectable liraglutide, which has a smaller small-molecule-specific advantage but still recruits the same circuit through the endogenous-receptor-binding mode.
The structure of the result matters. The central amygdala is not where homeostatic intake is regulated. That is the hypothalamus and brainstem. The central amygdala is where the brain decides what to want. The Güler team did not just find that GLP-1 drugs reach a deep brain region. They found that GLP-1 drugs reach the specific region where motivation gets calibrated, and they found that the drugs reduce that calibration's bias toward high-calorie food.
What This Suggests About Side Effects and Off-Label Effects
Two clinical patterns now have a candidate mechanism. The first is the reported reduction in alcohol and substance use among GLP-1 patients. The pharmacoepidemiologic signals from Wang and colleagues in 2024 suggested lower rates of alcohol use disorder diagnoses and cannabis use disorder diagnoses among semaglutide users compared with matched controls. Those signals are not proof, but they are coherent. If GLP-1 drugs reduce dopamine release in the nucleus accumbens during a rewarding stimulus, the effect should not be specific to food. Drugs of abuse drive dopamine release in the same circuit. The same molecular brake should, in principle, work on them.
The second pattern is harder. A subset of GLP-1 patients describe a flatter overall affect — food tastes less interesting, hobbies feel less compelling, sex drive drops. This is uncommon but real, and it has been called "anhedonia" in lay coverage. If the central amygdala circuit Güler described is engaged not only by food but by other rewards, then a drug that durably dampens dopamine transients in the nucleus accumbens could blunt those experiences. Nothing in the mouse data demonstrates this in humans. Nothing in the mouse data rules it out either. The mechanism is plausible. Whether it explains the reports in clinic remains an open question.
For a previous PeptideKnow piece on a different downstream effect of the same general pathway — reduced romantic motivation among some GLP-1 users — see our May 10 coverage. The Godschall et al. paper is the cleanest mechanistic substrate published so far for that family of reports.
The Drug-Design Question
One of Güler's stated next steps is the obvious one: design molecules that engage the appetite circuit without engaging the reward circuit, or the other way around. The two effects sit in different anatomical regions. They are in principle separable. Whether they are in practice separable depends on the receptor pharmacology — whether ligands can be engineered with biased signaling that activates one downstream pathway preferentially — and on whether the same GLP-1 receptor produces different cellular effects in different cell types.
The therapeutic upside of separation runs in two directions. A drug that suppresses reward but not appetite would be a tool for substance use disorder without weight loss. A drug that suppresses appetite without touching reward would be a weight-loss drug without the "things stop feeling fun" risk. Neither molecule exists yet. The Godschall paper makes both more plausible to pursue.
For chemists, the more immediate consequence is that the tryptophan-33 contact, which gates small-molecule efficacy at the human receptor, is now a known anchor point. Medicinal chemistry programs already use it. The paper does not change the drug-design playbook in a fundamental way; it characterizes what the playbook has already produced.
Caveats Worth Naming
These are mouse data. Even with humanized receptors, the rest of the mouse brain is mouse. Reward circuitry in mice and humans share architecture but differ in detail. Dopamine release dynamics measured by fiber photometry are not directly comparable to whatever a human reward-related experience looks like. The team is appropriately careful about this in the paper itself.
The cell population in the central amygdala is small. The conditional manipulations work by Cre-driver lines that target neurons defined by GLP-1 receptor expression. Off-target expression in those drivers is always possible. The team triangulated across multiple approaches — optogenetics, chemogenetics, viral re-expression, conditional knockout — which reduces but does not eliminate that concern.
Finally, none of these data establish the long-term effects of chronic GLP-1 dosing on this circuit. Acute and short-term manipulations may not predict what happens to the central amygdala under months or years of receptor engagement. That is the open question with the most clinical bite, and it is the one a mouse study cannot answer.
What This Means for Different Audiences
For prescribers: the paper does not change current prescribing. It does provide a mechanistic frame for patient reports that previously seemed disconnected from the drug's primary indication — reduced alcohol use, blunted enjoyment of food, occasional reports of flattened affect. Those reports now have a circuit they map onto.
For patients on these drugs: the experience of food tasting less interesting is consistent with what the drug is doing in the brain. It is not imagined. Whether the effect generalizes to non-food rewards varies between people. If it does and it is unwanted, that is worth raising with the prescriber.
For the broader peptide and metabolic-disease audience: orforglipron's April 1, 2026 FDA approval as Foundayo was a market event. This paper is the scientific follow-up to that event. It is the most detailed account so far of what the small-molecule oral GLP-1 class is actually doing in the brain.
Frequently Asked Questions
Does this mean GLP-1 drugs cause depression?
The data do not say that. They say that a GLP-1 drug reduces dopamine release in the reward circuit during a rewarding meal in a mouse. That is a different statement than "the drug causes depression." Depression is a clinical syndrome with multiple features, only one of which is reduced reward responsiveness. The pharmacoepidemiologic data on depression in GLP-1 users have been mixed and do not show a clear effect either way. The mechanism described here is consistent with a subset of reports of blunted affect among patients but does not establish a depression risk.
If GLP-1 drugs work on reward, should they be used for addiction?
Trials are underway. The Wang et al. pharmacoepidemiologic signals suggested lower rates of new alcohol and cannabis use disorder diagnoses among semaglutide users. Active clinical trials are testing semaglutide and related drugs in alcohol use disorder specifically. The Güler paper makes those trials biologically more plausible but does not by itself establish efficacy.
Why orforglipron specifically?
Orforglipron is the first oral small-molecule GLP-1 receptor agonist approved by the FDA. It went to market in April 2026 as Foundayo. As an oral once-daily tablet, it is logistically easier to take than the injectables and substantially cheaper to manufacture. It is also non-peptide, which changes how it gets through the blood-brain barrier and which brain regions it reaches. The Güler team's central finding — that small-molecule GLP-1 drugs reach the central amygdala at meaningful concentrations — is most relevant to this class.
What about semaglutide and tirzepatide?
The paper used liraglutide as its representative injectable peptide GLP-1. Semaglutide and tirzepatide were not directly tested in the Godschall experiments. The mechanism is not exclusive to small-molecule drugs; the injectable peptides can also recruit the central amygdala circuit, though probably less effectively because of differences in brain penetration. The clinical reports of reduced reward responsiveness come predominantly from semaglutide users, suggesting the effect generalizes.
Where can I read the paper?
The full text is on the Nature website at doi.org/10.1038/s41586-026-10444-4. NIH's summary is at the NIH news release. The University of Virginia summary is here.
What is the next milestone?
Two things to watch. First, controlled human studies of GLP-1 effects on non-food reward — alcohol, gambling, palatability ratings of non-food stimuli — will start to translate the mouse circuit into human readouts. Second, medicinal chemistry programs explicitly aiming to dissociate appetite and reward effects will produce candidate molecules over the next two to three years. Neither has a guaranteed timeline.
Sources
- Godschall EN, Gungul TB, Sajonia IR, et al. "A Brain Reward Circuit Inhibited By Next-Generation Weight Loss Drugs in Mice." Nature. Published May 6, 2026. DOI 10.1038/s41586-026-10444-4.
- NIH news release: "Oral small-molecule GLP-1 drugs penetrate deep into the brain to suppress cravings," May 6, 2026.
- University of Virginia summary: "UVA Study Reveals How New Weight-Loss Drugs Reshape the Brain".
- GEN coverage: "Oral Small-Molecule GLP-1s Linked to Deep Brain Activity and Reduced Cravings in Mice", May 7, 2026.
- NeuroscienceNews coverage: "GLP-1 Drugs Found to Directly Rewire Brain's Reward System", May 7, 2026.
- Background on the tryptophan-33 species difference: Kawai T, et al. Proceedings of the National Academy of Sciences. 2020. PubMed listing: PMID 32576683.
- Pharmacoepidemiology of GLP-1 effects on substance use: Wang W, et al. Nature Communications. 2024. PubMed listing.
This article reports on preclinical research published in a peer-reviewed journal. Findings are in mice. Nothing here is medical advice. If you are taking a GLP-1 drug and have questions about its effects, ask your prescriber.
Sources & References
- FDA PCAC Meeting Announcement (July 23-24, 2026)
- PBS: FDA to Weigh Easing Limits on Peptides Favored by RFK Jr.
- BioPharma Dive: FDA Peptides RFK Advisory Committee Restrictions
- RAPS: FDA Considers Adding a Dozen Peptides to Bulk Drug List
- Ars Technica: RFK Jr. Forces FDA to Reconsider 12 Peptides
- ProPublica: Peptide Safety Investigation
- New York Times: Peptide Ban FDA RFK Jr.
- SSRP Institute: FDA Announces Change in Status of 12 Peptides
- CNBC: RFK Jr. Peptides Hims Hers GLP-1
- USA Today: RFK Jr. FDA Peptides Explainer


