
NIH researchers reported Friday that semaglutide's weight-loss effects in the brain depend on cyclic AMP signaling inside a small population of hindbrain neurons, and that some neurons sustain that signal while others let it fade. The team also showed they could nudge the fading neurons toward the sustained pattern by adding roflumilast, an approved PDE4 inhibitor used for chronic obstructive pulmonary disease. The result, published in Nature Metabolism on May 22, 2026, is a mechanistic look at why GLP-1 drugs work the way they do — and a clue to why responses to those drugs vary so much from person to person.
This is not a clinical trial. It is mouse brain tissue, imaged over hours, in a study designed to look at signaling rather than weight change. The combination of semaglutide plus roflumilast was not tested in animals or people for weight loss. What the paper offers is a candidate explanation, with an obvious next experiment attached. The next experiment is what makes the paper interesting to anyone outside neuroscience.
What the Study Actually Showed
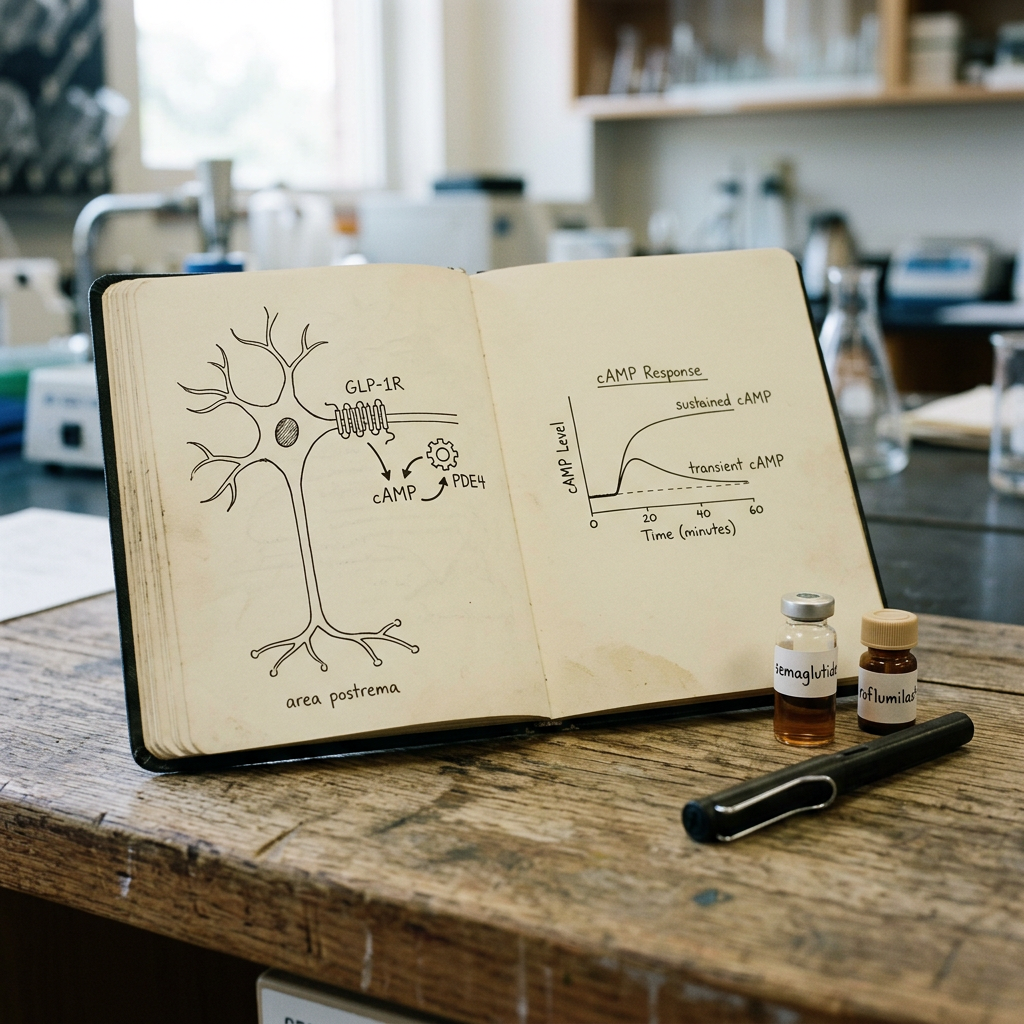
Claire Gao, a postdoctoral fellow at NIH's NIGMS and first author on the paper, led the imaging work. The group, co-corresponding authors Andrew Lutas at NIDDK and Michael Krashes also at NIDDK, used a fluorescence indicator to watch intracellular cAMP rise and fall in living brain slices from mice. The slices came from the area postrema — a chemosensory region of the brainstem, sitting just outside the blood-brain barrier, that is known to express GLP-1 receptors and to drive nausea, malaise, and food aversion when GLP-1 agonists hit it.
When the researchers applied semaglutide to those slices, cAMP went up in GLP-1R-expressing neurons. The size and duration of that rise was not uniform.
"It was not an all or nothing phenomenon. We observed that cAMP responses across cells varied on a continuum," Krashes said in the NIH announcement. Some neurons held their elevated cAMP steady. Others let it taper off. The paper's interpretation of the difference is that the tapering neurons may be internalizing or degrading their GLP-1 receptors more aggressively, so even with semaglutide still present in the extracellular space, the intracellular signal fades.
The PDE4 manipulation is the part that ties this to drug discovery. PDE4 is a phosphodiesterase — an enzyme that hydrolyzes cAMP, ending the signal. Roflumilast blocks PDE4, which keeps cAMP elevated longer. When the team added roflumilast on top of semaglutide, the population of neurons shifted: fewer tapering, more sustained. The pharmacological lever moved the biology in the predicted direction.
Why a Signaling Paper Matters for the GLP-1 Era
Three years into the GLP-1 obesity boom, the open clinical questions are no longer about whether these drugs work. They work. The questions are about variation, plateau, and durability.
Variation: roughly a third of patients on semaglutide or tirzepatide in post-marketing cohorts respond modestly or not at all, even at maximal doses. Plateau: most patients who lose substantial weight stop losing it at some point, often before they reach their target. Durability: when patients stop the drug, weight comes back. None of those observations has a clean mechanistic explanation. They are usually attributed, in handwaves, to "individual differences in GLP-1 signaling" without much specificity about what that means at the receptor or pathway level.
Gao's paper hands the field a specific, testable piece of biology underneath the handwave. If real interpatient variation in semaglutide response tracks with the proportion of area postrema neurons that sustain versus taper their cAMP response — a question that mouse genetics and human imaging could in principle address — then the plateau and the non-response phenotypes start to have a concrete cellular address. And if PDE4 inhibition moves the population toward sustained signaling, the path to a combination therapy becomes obvious in shape, if not yet in execution.
About Roflumilast
Roflumilast is not a peptide. It is a small molecule PDE4 inhibitor, sold under the brand name Daliresp, approved by the FDA in 2011 for severe COPD with chronic bronchitis to reduce exacerbations. Its profile in humans is well characterized: it works, it produces meaningful weight loss as a side effect (a fact pharmacologists noticed years ago), and it has GI side effects of its own — nausea, diarrhea, weight loss in some patients beyond what the COPD trials targeted.
The weight loss signal in COPD patients is what makes the NIH paper resonate with the GLP-1 community. If roflumilast already produces weight loss on its own, and if it potentiates GLP-1 signaling in the brain region most associated with semaglutide's CNS effects, the combination has the texture of a hypothesis worth testing in animals quickly. Whether it survives that test is a separate question. Combination biology is full of cases where two drugs that look additive in a slice preparation deliver less in vivo, or deliver too much of the wrong thing — in this case, too much nausea, since the area postrema is also the seat of GLP-1-induced anorexia and emesis.
The NIH researchers explicitly flagged this caveat. Their imaging captured hours of signaling. Weight loss happens over weeks and months. They said in the announcement that they intend to extend the imaging timeline to days and weeks before drawing translational conclusions. That is a much more careful framing than the press release headline suggests.
Why the Area Postrema, Specifically
To a neuroscientist, the area postrema is a strange place to study a weight-loss drug. It is best known as a vomiting center, one of the few regions of the brain where the blood-brain barrier is permeable, so it can sample circulating chemistry and trigger emesis when something looks toxic. Many of the side effects patients hate about GLP-1 drugs — the nausea, the food aversion, the early satiety — trace back here.
But the area postrema is also dense with GLP-1 receptors, and dense with circuit projections to the nucleus tractus solitarius and on to hypothalamic feeding centers. Recent work from several labs has rebuilt the older picture, in which GLP-1 drugs worked mostly through the hypothalamus, into a newer picture in which the hindbrain — area postrema and adjacent nuclei — does much of the heavy lifting. A March 2026 paper on orforglipron and the central amygdala argued that reward-circuit modulation matters too. An April paper on dopamine and pair bonding hinted that GLP-1 effects extend into social motivation. The current Gao paper does not contradict any of that. It locates one piece of the mechanism with new resolution.
Carl Zimmer-style aside: the picture starting to come together looks less like a single switch and more like a thermostat in a house with several thermostats. The area postrema responds to the drug, sets the appetite signal, and depending on which neurons sustain that signal and which let it fade, the system reaches different equilibria. Some houses cool down a lot. Others barely change temperature. Tweaking PDE4 nudges more thermostats toward holding their setpoint.
What This Paper Does Not Show
The careful reader of an NIH press release develops habits. The first habit is to check whether the in vivo behavior matches the in vitro mechanism. It does not, here. Nobody has yet shown that adding roflumilast to semaglutide produces additional weight loss in mice, let alone in people. The slice imaging is consistent with that hypothesis. It is not evidence for it.
The second habit is to check whether the species and the model translate. Mouse area postrema neurons and human area postrema neurons share architecture but not necessarily quantitative pharmacology. The dose range, the receptor density, the PDE4 expression pattern, all of these could differ. The fact that roflumilast already produces weight loss in human COPD trials is the closest we have to a human translational signal, and it is suggestive rather than confirmatory.
The third habit is to check whether the proposed combination would be safe. PDE4 inhibitors have a real GI side effect profile. GLP-1 drugs have a real GI side effect profile. Adding them together in a brain region that controls nausea is exactly the kind of experiment that could produce a drug intolerable for the patients who most need it. The Phase 1 design for any combination study would have to be very careful with titration.
The fourth habit is to ask who benefits commercially. Roflumilast is generic. AstraZeneca, the original developer, no longer has IP cover. A combination of semaglutide and roflumilast would not be a product Novo Nordisk could easily protect. The mechanism is more likely to feed next-generation PDE4-aware molecules — perhaps PDE4D or PDE4B selective inhibitors, perhaps brain-penetrant analogs — than to launch a roflumilast revival in obesity.
How This Could Shape Next-Generation Peptide Design
The implication that excites peptide chemists is not the roflumilast combination per se. It is the receptor-trafficking observation underneath it. If some neurons taper their cAMP response because they internalize or degrade GLP-1 receptors, then peptides that engage the receptor in ways that minimize internalization should sustain signaling on their own. This is a known design problem in GPCR pharmacology, with a body of literature around "biased agonism" — molecules that engage the receptor at the cell surface but minimize the intracellular machinery that pulls the receptor into endosomes.
That framing suggests two parallel paths for next-generation GLP-1 design. First: peptide modifications that bias signaling toward sustained cAMP at the surface rather than rapid receptor internalization. Second: dual-mechanism molecules that pair GLP-1 receptor agonism with PDE4 inhibition in a single agent, or that pair GLP-1 agonism with other intracellular signal-stabilization machinery. Neither is straightforward chemistry. Both have at least decade-long precedent in the receptor pharmacology literature for other GPCRs, which is encouraging.
For the GLP-1 dual and triple agonists already on the market or in late-stage trials — tirzepatide, retatrutide, the freshly reported TRIUMPH-1 data — the cAMP-trafficking framework offers a way to talk about why retatrutide's effect size at 80 weeks was so large. A triple agonist activates three different receptor populations across the brain. If each of those populations has its own cAMP-sustaining versus tapering distribution, hitting three receptors instead of one improves the odds of pulling a given patient into the sustained response on at least one mechanism. The triple-agonist hypothesis becomes, in part, a hypothesis about hedging against receptor desensitization.
The Bottom Line
A short paper, a single laboratory's mouse data, an old generic drug, and one mechanism explanation. That is what NIH announced Friday. None of it changes prescribing patterns next week. None of it changes a patient's response to semaglutide today.
What it does is put a specific cellular handle on the variation, plateau, and durability problems that have shaped how clinicians talk about GLP-1 drugs since the obesity boom began. And it offers a candidate combination — PDE4 inhibition layered onto GLP-1 receptor agonism — that the field can now test in animals and, if those experiments hold, eventually in people. That is a meaningful contribution. Not a breakthrough. A clean handhold on biology that was previously a black box.
Frequently Asked Questions
Does this mean roflumilast can make my semaglutide work better?
No. This is mouse brain tissue, imaged over hours. No animal weight-loss experiment has been done with the combination yet, let alone a human one. Patients should not combine prescription drugs based on a mechanistic paper. Both drugs have meaningful GI side effects, and combining them outside a clinical trial could produce intolerable nausea or worse.
What is cAMP and why does it matter here?
Cyclic AMP is a small intracellular molecule that GPCR signaling produces and uses to relay receptor activation to the cell's machinery. When semaglutide binds its receptor on the outside of a neuron, the receptor signals the inside of the cell partly by making cAMP. If cAMP stays up, the signal stays on. If an enzyme called PDE4 chews it back down, the signal fades. The paper is essentially showing that PDE4 sets the timer on how long semaglutide's intracellular signal persists.
Where is the area postrema and why does GLP-1 hit it?
It's a small region at the back of the brainstem, in a strip where the blood-brain barrier is unusually permeable so the brain can sample circulating blood directly. That position lets it detect things like toxins, which is why it's also a major vomiting center. It's loaded with GLP-1 receptors, which is why GLP-1 drugs produce nausea, food aversion, and meaningful appetite suppression by acting there.
Why might some neurons sustain cAMP while others don't?
The paper's interpretation is that the tapering neurons may be pulling their GLP-1 receptors off the cell surface — internalizing them, sometimes degrading them — even with semaglutide still around. That receptor trafficking is a known phenomenon for GPCRs broadly. The neurons that sustain cAMP probably do less of it, or recover their receptors faster, or both.
Does this explain why tirzepatide and retatrutide work better than semaglutide?
Indirectly, maybe. Activating two or three different receptors instead of one means three different cAMP timecourses are layered on top of each other in three different brain populations. If receptor desensitization is the rate-limiting step in a single-agonist drug like semaglutide, then hitting more receptors at once is one way around it. The Gao paper doesn't make that claim, but the implication is sitting there.
Sources
- Gao C, et al. "Semaglutide drives weight loss through cAMP-dependent mechanisms in GLP1R-expressing hindbrain neurons." Nature Metabolism. 2026.
- NIH National Institute of Diabetes and Digestive and Kidney Diseases. "NIH researchers identify avenue for enhanced GLP-1-induced weight loss." NIH.gov news release. May 22, 2026.
- US Food and Drug Administration. "DALIRESP (roflumilast) tablets, for oral use — full prescribing information." FDA label, 2018.
- Wilensky LH, Williamson SD, Kantar PJ. "Roflumilast for chronic obstructive pulmonary disease." Cochrane Database of Systematic Reviews. 2017.
Sources & References
- FDA PCAC Meeting Announcement (July 23-24, 2026)
- PBS: FDA to Weigh Easing Limits on Peptides Favored by RFK Jr.
- BioPharma Dive: FDA Peptides RFK Advisory Committee Restrictions
- RAPS: FDA Considers Adding a Dozen Peptides to Bulk Drug List
- Ars Technica: RFK Jr. Forces FDA to Reconsider 12 Peptides
- ProPublica: Peptide Safety Investigation
- New York Times: Peptide Ban FDA RFK Jr.
- SSRP Institute: FDA Announces Change in Status of 12 Peptides
- CNBC: RFK Jr. Peptides Hims Hers GLP-1
- USA Today: RFK Jr. FDA Peptides Explainer


